
From Strained to Strength: Achilles Recovery
The Achilles tendon is well-known because of its association with the Greek hero - Achilles. Greek mythology paints Achilles as an invincible warrior dipped into the River Styx, leaving only the heel where he was held vulnerable to harm. His story is epic. He slayed so many men in battle, even defeating the Trojan prince Hector, before being taken out by a god’s guided shot to the ankle. Unfortunately for us humans, we are not invincible, and therefore have a higher probability of experiencing many injuries. Though as luck would have it, the likelihood that an Achilles injury will kill us is pretty slim.
Achilles tendon injuries can be painful, though, and the recovery can take up to a year or more! Whether you’ve experienced a strain or a full tear in this tendon, you know how difficult it can be to rehabilitate. If you are someone dealing with Achilles pain, take comfort in knowing that healing is possible, even post surgery. Just like any other issue, the right tools and providers are needed to assist you.
Since my specialty at Solstice Massage Therapy is neuromuscular therapy, I will mainly be focusing on that approach. Massage can do so much for the Achilles tendon; manual work can help prevent an injury or it can help during recovery and even post surgery by releasing tension in the surrounding muscles, creating greater range of motion for the Achilles tendon, and even assisting the drainage of the synovial fluid that causes swelling behind the ankle.
What is the achilles tendon?
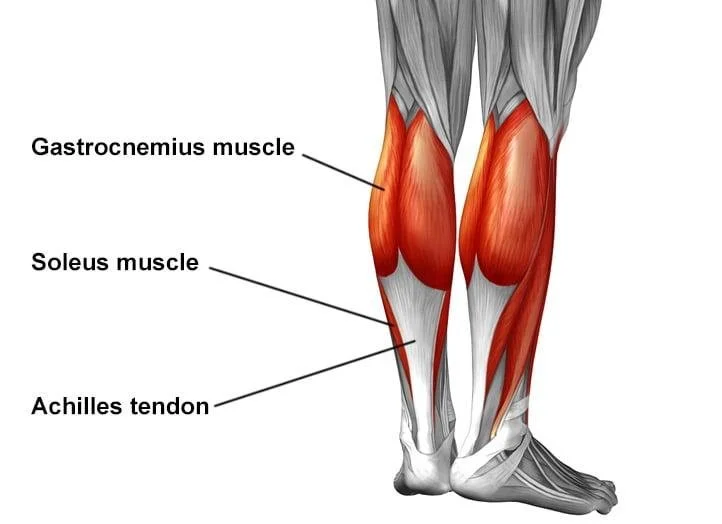
The tendon is nicknamed ‘Achilles’ due to the Greek story I previously mentioned, but its anatomical name is actually the calcaneal tendon. It is a thick band that connects the calf muscles (gastrocnemius and soleus) to the heel (posterior surface of the calcaneal bone).
Being made up of dense, regular connective tissue, it is the largest and strongest tendon in the human body - though it is heavily loaded, meaning it is repetitively subjected to immense mechanical stress. Its collagen fibers allow for flexibility and strength while walking, running, jumping, and absorbing and releasing force. The calcaneal tendon’s primary job is plantarflexion, or pointing the toes downwards. When we walk, we repeat this motion several times per day while combating the force of human locomotion. The calcaneal tendon acts like a spring if you can imagine it. It stores and releases elastic energy, and can even withstand 10 -12 times the weight of the human it’s carrying while exerting said force. The calcaneal tendon also stabilizes the ankle and assists with balance.
How Injuries Occur
If it’s true that the Achilles tendon can withstand so much force, why is it one of the most common injuries among athletes, weekend warriors, and workout enthusiasts?
Many factors can contribute to causing an Achilles tendon injury. First of all, the tendon can be irritated but not torn, which usually results in pain and swelling, and can be healed with rest. A rupture is a much more serious injury. Let’s explore some of the reasons responsible for an injured Achilles tendon.
Overuse - activities like running, jumping, sudden increases in training volume, and explosive sports can overload the tendon faster than it can adapt.
Limited ankle mobility - poor mobility changes how force moves through the ankle and can increase strain on the Achilles.
Tight or weak calves - If the gastrocnemius and soleus become overly tight, the lower leg loses mobility. That restriction changes how force moves through the Achilles tendon. This means the tendon must compensate for the muscles lack of movement, which limits the amount of force the tendon can absorb. If the gastrocnemius and soleus are weak, on the other hand, the effect is a reduced load-bearing capacity. This leads to structural changes such as thinning and decreased stiffness. In other words, the Achilles tendon is not properly supported and therefore the chances of an injury are much higher
Poor load management - if the expectation for the Achilles is greater than the function of the muscle itself, injury can occur. For instance, someone in their 40s that is not regularly training to defeat the Trojan army would have a much higher chance of straining the tendon compared to someone who appropriately cares for their tendon and knows when not to push it. These injuries often happen when activity levels suddenly exceed what the body has been prepared for.
In the case of a strain in the Achilles, there would be pain, swelling, and possibly even bruising from the microtears in the tendon. A rupture, however, would be incredibly painful and would result in a trip to the emergency room. Depending on the severity of the tear, surgery may be recommended.
What is a Calcaneal Rupture?
Calcaneal tendon ruptures are serious injuries that require a medical diagnosis. Expect a referral to an orthopedic specialist; they will do various tests to determine the severity of the tear. The difference in care and recovery depends highly on the degree of the rip: if it is a partial tear, usually surgery is not required but if it is a full tear, surgery to reattach the two pieces will more than likely be necessary. Sometimes a functional rehabilitation plan sans surgery is possible.
Full Rupture: When the Achilles tendon is torn, the result is a sudden popping noise, followed by severe pain and immediate loss of function if the tear is a full rupture. This means the tendon is completely torn in two and the gastrocnemius and soleus are no longer connected to the calcaneal(ankle) bone. The foot will feel “floppy” and the injured person will not be able to point their toes, nor will they be able to push off the toes to walk. Flexion of the toes will be impossible. Recovery for a full tear is about 6 to 12 months. So not death, but still pretty inconvenient if you’re trying to fight the Trojan army.
Partial Rupture: While still a serious injury, it does not require surgery, as only some of the fibers have been torn. When torn, there will be a sudden pain at the back of the ankle, with swelling and bruising. Walking will be possible but incredibly painful, and pushing off the toes or flexing of the toes/foot will feel weak. Recovery usually takes about 3 to 6 months.
No matter the degree of pain, if you think you’ve torn your Achilles tendon, it is imperative that you visit either a walk-in clinic or an emergency room post haste. Holding off on treatment and diagnosis can affect the healing time needed for a calcaneal rupture. An orthopedic specialist will perform the Thompson test: the affected person lies down while the doctor squeezes the calf. If the toes move reactively to this, it indicates that the tear is partial. Most likely, an MRI will be necessary as well.
Massage Therapy for the Achilles Tendon
If you wish to receive massage therapy after dealing with an Achilles tendon rupture, you will have to get cleared for massage by your surgeon or orthopedic specialist before doing so. How quickly you’ll be able to utilize massage fully depends on whether or not surgery was needed and what kind of massage you’re wanting. Crucially, avoiding aggressive work on the rupture site, and respecting healing times are the key principles here.

Lymphatic Drainage: great for swelling and bursa sac fluid buildup. Lymphatic drainage is a light pressured massage, and the goal is to aid in circulation and, oddly enough, lymphatic drainage. This can sometimes be cleared 2-3 weeks post injury; the pressure is light enough that there is no danger of re-rupturing the tendon, and the drainage and swelling reduction can help with the pain and the healing timeline.
Scar Tissue Massage: allowed sometimes as early as week two, but only if the surgeon has signed off on it and the incision is fully closed.
Myofascial Massage: since this work is gentle and slow, myofascial work can be cleared in the 4-6 week time period by a surgeon or physical therapist. At this point, deep work or pressure directly on the incision site should be avoided. Working with the superficial fascia is wildly helpful for keeping the gastroc and soleus muscles flexible and lubricated. The reduction in fascial adhesions and increase in circulation at this point can go a long way to lowering pain levels and complimenting physical therapy in the healing process.
Therapeutic Massage: known as “deep tissue”, therapeutic massage means any type of modality using more pressure or working with deeper muscles. This should be avoided until at least week 12 with, you guessed it, a doctor’s note to clear the injury for massage. I would exercise caution with more aggressive types of massage, such as sports massage or rolfing, but at this point, neuromuscular therapy would be safe as long as you have a knowledgeable provider, which is my specialty!
How Massage Supports Healing
Once the initial healing phase has passed, this is where massage therapy can become especially helpful. After the first 12 weeks are up, I’d recommend massage to aid in your recovery and assist the physical therapist in regaining function, range of motion, and getting you back to your daily activities or sports that you love. At this point, and honestly up until your recovery is at a point where you almost never have pain, I would avoid direct firm pressure right above the ankle. There is just no point in risking a re-rupture. Besides, it’s more effective to work on the compensation patterns, the gastrocnemius and soleus muscles, and assist in bursa sac fluid movement anyway.
Here’s a breakdown of the muscles I address for Achilles tendon recovery. I like to start anteriorly because it is likely that these muscles have been compensating for the lack of mobility in the Achilles and subsequently the gastrocnemius as well. I find that working with these muscles first decreases tension so the posterior muscles have the space to rehabilitate as well. It also greatly helps the nervous system get accustomed to my presence and makes working with the injury that much easier.
Anterior lower leg protocol:
Starting with the flexor digitorum longus, I use a medium amount of pressure, starting just above the malleolus and moving proximally (toward the knee). I have the client perform medial flexion and lateral dorsiflexion, intertwined with rest, in order to create change. I then move to the peroneus muscle and have the client do the same motion. These muscles aid in plantar flexion and help stabilize the lower leg, so they will be overused at this point in recovery.
Then moving onto the extensor digitorum longus and the tibialis anterior. Both these muscles are direct antagonists to the gastrocnemius and soleus and will be needing attention. Using a medium to a moderate pressure, I would start just below the patella and move distally this time, while having the client perform dorsiflexion and plantarflexion. If Achilles tendon rupture prevention is your goal, having work done here is crucial; when this muscle is overly tight, it dorsiflexes the toes at rest (raises the toes) which will pull on the Achilles tendon and may even contribute to knee tension.
Posterior lower leg protocol:
Moving to the gastrocnemius and soleus now, I start with soothing strokes to introduce my presence and palpate any trigger points, as well as check range of motion. Before I add pressure, I like to see how the lower leg is responding to movement and light touch. I want to see how the fascia is sitting above and around these muscles and if it will allow for manipulation. It is likely that I’ll have to begin with a bit of myofascial release before jumping straight into neuromuscular therapy. Using medium pressure, I would work proximally starting at the base of the gastroc, NOT at the Achilles tendon. The client would dorsiflex, then plantarflex, then rest and repeat until the pressure made it to the top of the gastroc and soleus. This would have to be performed a couple times on each side, more or less reps depending on the severity - whether or not surgery was needed and how long it had been since the injury.
At the calcanean bone attachment and bursa sack, effleurage is used for synovial fluid movement. Light pressure only is what is required here, along with strokes moving proximal to the foot in order to encourage the fluid to move out of the bursa sac and reduce swelling.
If you are someone who loves a visual, I have a video on my socials that detail my process for working with the Achilles tendon. You can find that here.
The goal here isn’t to force a change and have you up and playing flag football the next day. We are working as a team to release the tension built-up in your muscles and trauma in your nervous system to allow change to happen. Massage most certainly can help reduce the guarding of the area, restore movement confidence, and improve circulation. Achilles bodywork is something that will need to be repeated diligently in addition to physical therapy exercises for long lasting change to happen, especially when dealing with a full tear situation.
Common Mistakes People Make in their Achilles Tendon Recovery
This tendon carries so much weight and force that it is easy to overdo it before or after recovery. I don’t want to scare you, but it is possible to tear the Achilles tendon twice. That is why having the right recovery plan is so important, along with avoiding these four things:
Stretching too aggressively too soon
Ignoring pain signals
Returning to activities (sports, running, etc) too quickly
Treating symptoms but not load capacity
Final Thoughts
Healing the Achilles tendon after an injury takes time and patience, but it can be done. With the right treatment plan, proper rehabilitation, and bodywork that respects the healing process, many people are able to return to the activities they love with greater confidence and less pain. Thankfully, a ruptured Achilles tendon probably won’t kill you, but it will test your discipline when it comes to self-care. If you’re dealing with Achilles tendon pain or bouncing back from an injury, I can build a plan that supports your recovery in a way that feels safe, collaborative, and sustainable.